Overall
Diagnosis
Treatment
Overall
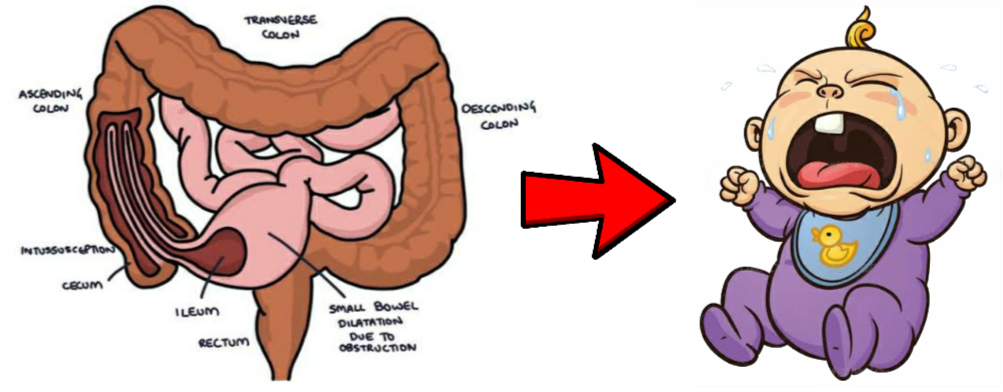
Telescoping of one part of intestine into the other the commonest is from proximal to distal.
Causing blocked of material which flow through the bowel as well as blood flow which can cause necrosis.
It is a serious condition. Common in the infants, 5 to 9 months of age.
TYPE
- Jejuno – ilial
- Jejuno jejunal
- Ilio – ilial
- Colo – Colic
- Retrograde jejunogastric
CAUSES
CHILDREN:
- During weaning period the intestinal pair patches get hypertrophied, as the baby consumes food other than milk. These hypertrophied lymph nodes partially obstructs the intestine and the peristalsis more in the proximal part and less over the distal part. Due to unequal in movement the proximal part of intestine which is moving more enters to the moving less part that is distal part
- Upper respiratory tract infection
ADULTS:
- Meckel’s Diverticulum
- Polyps
- Tumours
- Submucous lipoma
- Carcinoma colon
- Weight loss surgery (Gastric bypass)
- Crohn’s Disease
PREDISPOSING FACTORS
- Upper respiratory tract infections
- Haemophilia
- Henöch-Schönlein purpura
- Cystic Fibrosis
- Coeliac disease
SYMPTOMS
- Sudden colicky abdominal pain with facial pallor
- one attack of red currant jelly stool
- In between two attacks the baby is absolutely normal but get up suddenly with pain
- Red currant jelly stools are not found in adult
- Pains start suddenly the baby stops playing and cries loudly, pressing and bending the affecting area
- Vomiting 3-4 times
- Constipation
- Feature of dehydration is not marked
- A sausage shaped mass seen around the umbilical region
- In case colo colic variety abdominal palpation shows dialated mass over the abdomen
- Weakness
- Step ladder peristalsis present
- Apex of intussusception shows in case of colo-colic variety in per rectal examination
- In untreated cases peritonitis seen
Diagnosis
INVESTIGATION
- Barium Enema
- CT scan ( Computerized Tomography)
- USG (Ultra Sonography)
Treatment
- It is emergency condition, immediately consult with doctor
- If the pain is continued, surgery is required – Laparotomy followed by opening the intussusception by manual traction
- If some portion of gut non-viable, resection anastomosis is perform
- Diet habit has to be changed that is milk to be started again and slowly shift over to other diet
- In case of intussusception is closed to the rectum water jet enema rapidly controlled the situation followed by change diet